The first day, I observed a hysterectomy, shadowed during his office hours, and watched him perform a circumcision. Day two was more office visits, plus rounding and learning how to suture; day three was office, plus learning how to gown and glove. I enjoyed it! His office was warm and charmingly decorated, his staff seemed happy to be doing their work with him, he talked at leisure with his patients, he spent very little time charting, and he was a kind teacher.
Whenever he found something pathological, he let me look (or feel!). I saw two cases of uterine prolapse, possible early vulvar and rectal cancer, a cervix s/p cone biopsy, and cervical blanching during colposcopy. We also mentioned Li-Fraumeni syndrome and cutaneous larva migrans, which had previously only been words and pictures on a page. I felt engaged and charged! I can get used to that.
My complete newness to physical diagnosis caused some amusing episodes, like when he told me to feel a patient's thyroid:
Dialogue:
outer • inner
|
Actions:
purported • actual
| |
| Doctor | (to patient) Mind if she feels your neck? | |
| Patient | No, not at all! | |
| Me | Thank you. Right. So... The thyroid gland is supposed to be here somewhere...does she have one? I guess it'd be here... (to patient) Please swallow. | Thyroid exam. Mimes a thyroid exam. Feels...a neck? |
| Doctor | I don't know about this kid... Left or right? | |
| Me | What is he talking about? Does she only have half a thyroid gland? I obviously didn't pick that up... Well... I have a 50/50 chance... Left. | |
| Doctor | You are fooling nobody. Good. It's like a little pea, moving under your fingers. (to patient) Swallow. | Puts my hand back on the patients neck, beneath his. Presses (hard). |
| Me | Good grief. Oh, cool. | Feels the thing for the first time. |
 |
| Tweezers, but you can bill more if you call them "pickups" (jk). After a few minutes of touching the needle in my bare left hand, I said aloud to Dr. C, "this can't be right," and he got me these. |
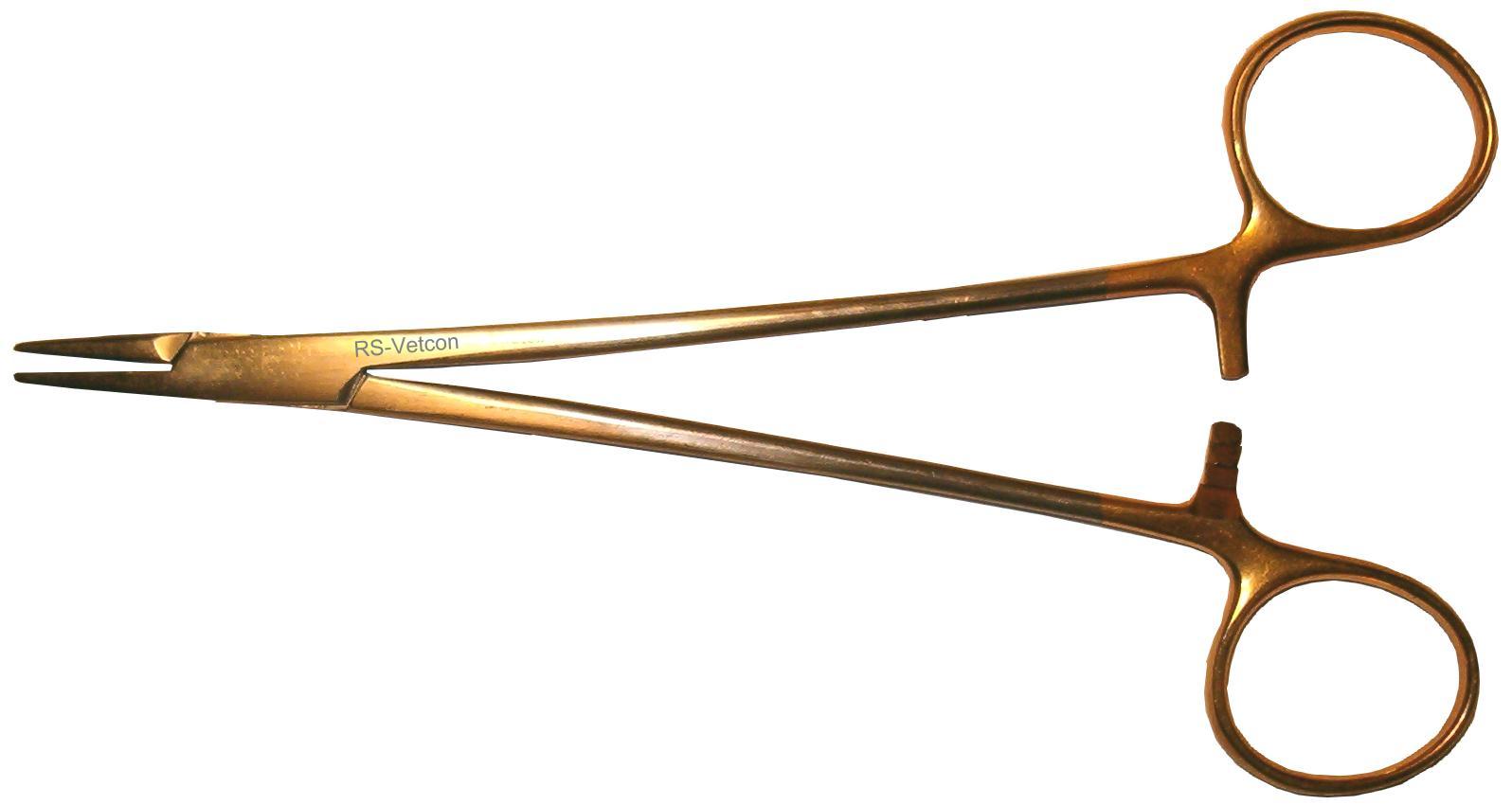 |
| Needle driver/holder. This thing is well-
designed. The short effector side of the lever (left) magnifies the force you place at the affector side (with scissor handle and locking mechanism). |
I'm clumsy with suturing and gloving. (It's all about muscle memory.) Dr. C gave me two pair of old pickups, a small needle driver, some expired ties, and opened suture so that I can practice. He also gave me three pair of unpackaged ("contaminated") sterile gloves and an opened gown. How generous of him! Someday, all these things will be second nature to me. I can get used to that.
I did get good at finding fundal heights and fetal positions. I made mistakes, but by and large (even in a primagravid uterus!) I could make out where the baby's head, buttocks, and back were located.
This doesn't matter during most of pregnancy (only at 30 weeks and on). However, you look slick if you find the baby's back, guesstimate where his heart is, and place the fetal doppler RIGHT on the spot. The result: immediate, deafening, staticky heartbeat to the delight of the mother and the attending. I can get used to that.


 That's funny.
That's funny.