This is as much a psychological milestone as it is a spiritual one. Human beings can't influence most of what happens to them: we can't change the weather, we can't change history, and we can't change the people around us or their choices. Christians embrace this like they embrace the inevitability of suffering: they see that God has made it a way to go to Him.
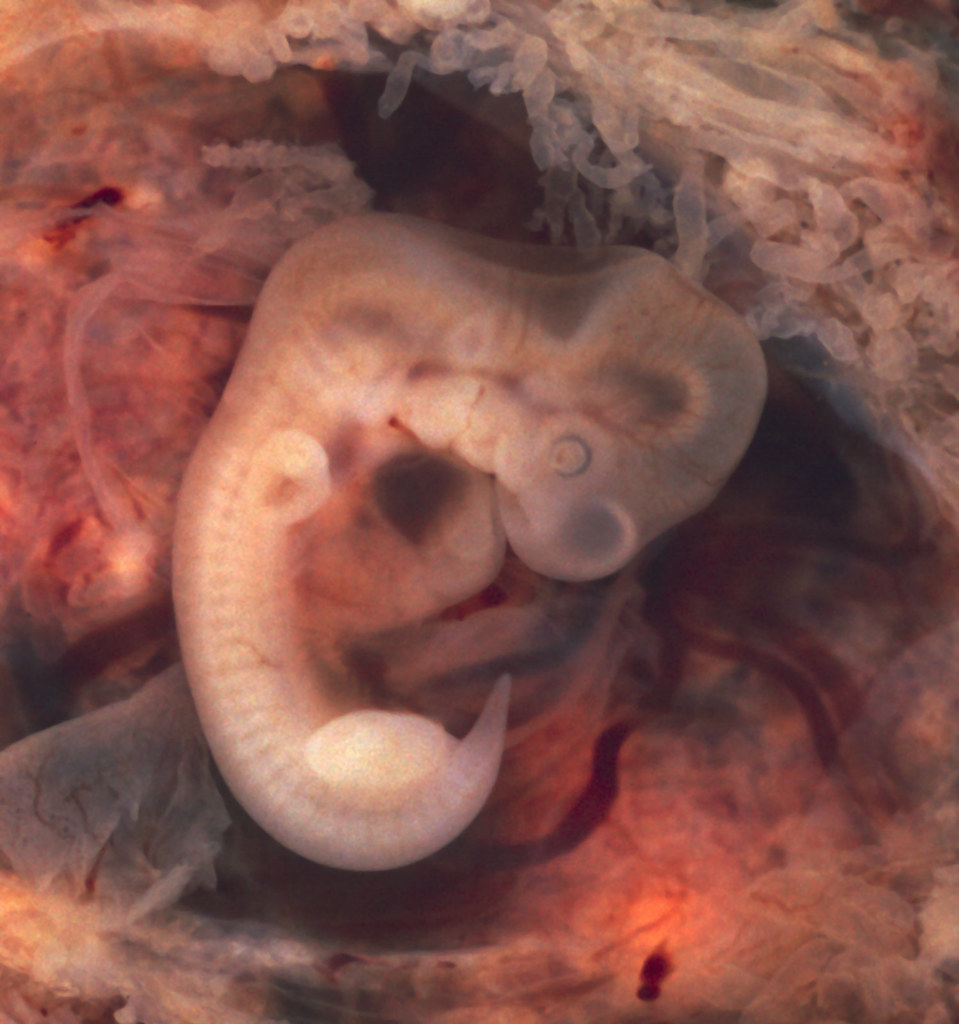
It's refreshing to admit I can't control a lot. As a doctor, I can't control who will page or call me and whether it means I get out of bed on call. I can't control who will walk into my clinic or how long they'll need to talk about it. I can't control who will come into triage or the ED and whether they'll need a complicated workup or a surgery that day. At the most extreme: I can't control how placentas and cancers grow and I can't stop babies and women from dying. There's a vulnerability that can be exhausting (another patient? I already need to see twelve. Another ultrasound? Another phone call?). It's hard to maintain generosity and avoid being lazy. Also increasingly since residency is the inability to control my body: I can't just stay up as long as I want--my body turns off after 36 hours on and I miss meetings that I schedule after that.
The doctor-patient coin has two sides. I can't control how my doctor interprets the evidence on re-scoping versus empiric titration. I can't control what she'll find on that colonoscopy, either. I can't control what the meds will do, I can't control whether I develop extraintestinal manifestations, and I can't control whether or when I'll lose my colon or get cancer. (I also can't control the past, which includes a lot of knowledge about UC that I sort of wish I didn't have.)
And there are a scattered other few things. I can't control whether my siblings will stay Catholic, whether my married friends will stay married, whether my archdiocese will close my parish, whether the state will stop payment from CMS to my hospital....
There are some things that I can control a little more, but always weasel out of my grasp. I can't always seem to control the cleanliness of my apartment. Sometimes it looks like six frat boys live there and I can hear my German-standard cleanliness mother (who had us wipe the microwave and oven doors as part of the list of things to do with the dishes) tsking in my mind. Mom, I think I've wiped the oven once and vacuumed three times since moving here.
Then there are the things I wish were in my control and might be in my control, but I don't think my will is disciplined enough. These are all the parts of the life of virtue that I think I could do better on, even though my life now in residency tempts me to excuse all kinds of stuff. I have to learn to live like a saint even while working my current schedule. What if I died in residency? What will be my excuse that I didn't possess my own heart in each moment, form my conscience, and use every opportunity to love God and calmly grow in virtue?
But my old approach to virtue doesn't work now. (Lots of people said this about med school, that they're undergrad method of studying didn't work in med school. I didn't have to make that transition from TAC, but perhaps it'd have been better if I did, because I'd have recognized this need for something new sooner.) I can't legislate little changes any more.

But the other day I had a realization. Considering the relationship between myself and God, I am never the legislator. God makes the laws and He stands under the reality in which I exert my free will with His help. This helped me realize what doctors of the Church and saints have long known: all that is needed for holiness is to follow one's conscience in each moment. When each opportunity to floss presents itself, I accept His grace and take care of my body. And because God's will is less totalitarian than man's, I might even decide (shocker) that flossing is not indicated in certain situations. (Do you floss after 30 hours at work? I fall into bed.)


















_2007-03-03.jpg)