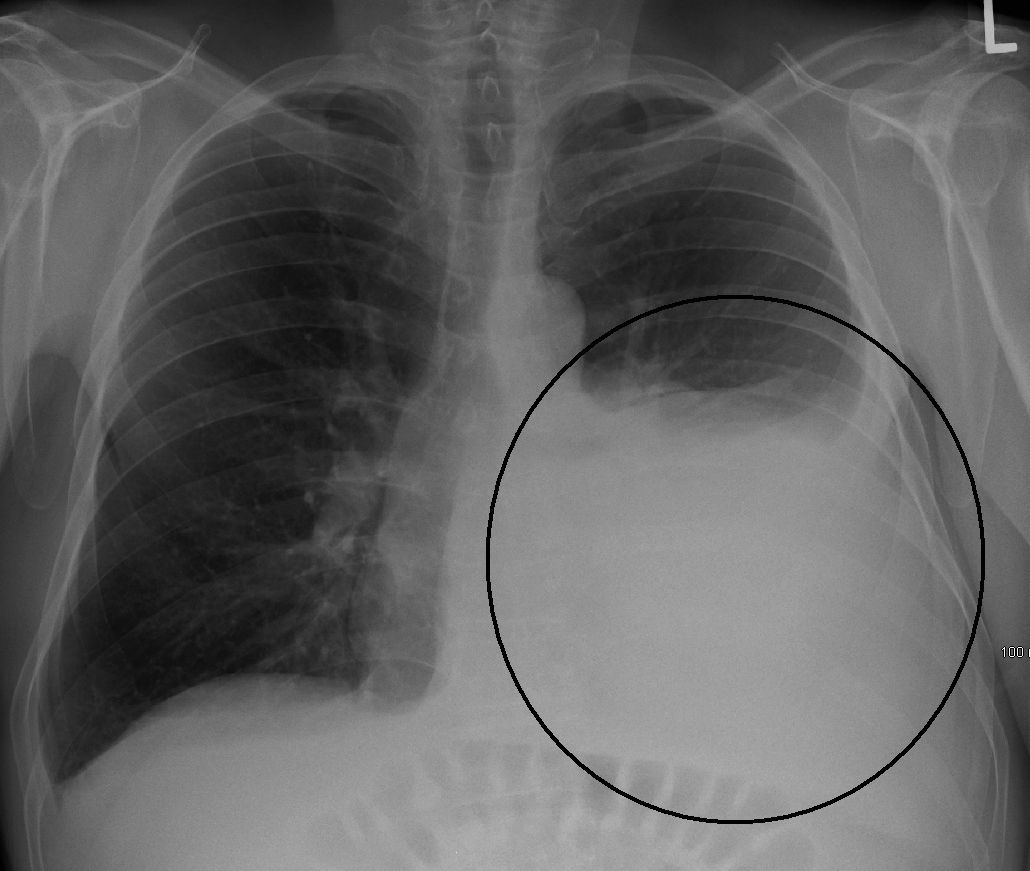
I am one week in to my second month of inpatient medicine, and I am run-down. I have seen a lot of sick people and learned a lot. It has been exciting, emotionally draining, and physically taxing. I wish I could tell you the story of the man with an enormous malignant pleural effusion, the story of the man with a hemoglobin of 1.8, the story of the man whose foot was amputated in the middle of the night, the story of the man with a failing heart, the story of the woman who presented with flu and was found to have leukemia, the stories of the several people found down, the story of the pregnant woman with flu, the story of the man with the three-foot aortic dissection, and the story of the man I thought was having a heart attack but who was really lying to me about his cocaine use....
I am one week in to my second month of inpatient medicine, and I am run-down. I have seen a lot of sick people and learned a lot. It has been exciting, emotionally draining, and physically taxing. I wish I could tell you the story of the man with an enormous malignant pleural effusion, the story of the man with a hemoglobin of 1.8, the story of the man whose foot was amputated in the middle of the night, the story of the man with a failing heart, the story of the woman who presented with flu and was found to have leukemia, the stories of the several people found down, the story of the pregnant woman with flu, the story of the man with the three-foot aortic dissection, and the story of the man I thought was having a heart attack but who was really lying to me about his cocaine use.... Daily Mass and meditation have been hard to get to, and that sends me into a tailspin of scrupulosity and humiliation. However, I was able to go Mass almost every day in the past week and formation is still going on. When you read this, please pray for my bishops; they are making some important decisions and need your help!
My schedule now looks like this:
4:50 Rise, MP
5:30 Drive to work
6:00-8:00 See patients and write notes
8:00-12:00 Round with resident or intern
12:00-1:00 Noon Conference with residents (Midday prayer doesn't happen during the week)
1:00-5:00 Lecture, studies, or other learning with resident or interns
7:00 Mass, EP
8:00 Home, mediation
9:00 Bed (NP doesn't happen much right now)
Unless I am on call (working 6:00-9:30), then I exempt myself from Mass and meditation.I am on call every fifth day, and this means that there are some days I work on Sundays and Saturdays. The day after call ("post-call") is also a workday, so if call lands on a Friday, I work Saturday (that happened this past week.) If call lands on a Saturday, I work Saturday and Sunday. The residents call this a "black weekend," but because of the way the call schedule works, it is always followed by a "golden weekend" of both Saturday and Sunday off. Obviously, when call was on Sunday once, I went to an anticipatory Mass.
_2007-03-03.jpg)
Two days before the call day, I am "on codes." A "code" or "code blue" is called when a patient goes into cardiac arrest. I carry a special pager on code days that goes off whenever a code blue is called, anywhere in the hospital. When that pager rings, it flashes where in the hospital the code is, and I immediately drop everything and walk/run there. I have been to three total, I think. There are usually plenty of people at a code, so I usually stand in the background. I gave chest compressions once. All three times, the person died. (The survival rate to hospital discharge from a code blue is extremely, extremely bad--don't let the medical dramas fool you.)
What does a medical student do in the hospital? I come early and see the patients assigned to me (usually three, yesterday four). I go into their rooms, (usually) wake them up, and ask them how they're doing. I follow up on their pain, nausea/vomiting, breathing, constipation/diarrhea, urine output, medicines, etc. Then I examine them. It's amazing how natural this is becoming! Then, I update them on any test results that I have seen and they haven't been informed about yet. I always leave big news for the resident or specialist, but if there is something simple I can tell them, I do. I ask them if they understand everything that's been told to them. Often, the answer is "no," and I know enough to help them understand. Then, I ask if I can do anything for them, and if not I leave and find a computer.

I submit my notes before 8:00, which is when the interns review my notes and see those same patients. They usually formulate their plan without taking mine into account (my notes are more for my education than the patient's care), but I have had some take some of my text and use it in their notes! Sometimes I round with them, but more often I join the "upper-level," a second-year resident. She has to see all the same patients again, too, because she checks the interns' work (and the attending physician checks hers). This is how doctors train! Daily practicing medicine with less and less supervision.
Noon conference is mandatory free lunch with lecture. Every day, we learn about something in medicine. I'm sure the upper-levels have heard some repeats, but repetition is the mother of learning. After noon conference, the med students have additional lectures and we also do practice questions or join the interns for some teaching. "Teaching" from a young doctor is different, depending on the doctor. With one of my interns, I trooped up to an ICU and we found a patient on a breathing machine so that he could give me a one-on-one mini lecture (with questions and practice cases all throughout it) on ventilator management. With another intern, we did practice board exam questions. With a third, I was left alone to read and do practice questions on my own.
As you can imagine, I'm learning a lot. This ended up being a respectably-long and mildly interesting post...I dive into IM again tomorrow and have a black weekend the next week, so I probably won't be blogging again soon. Pray for me, and for my bishops!